Prostate Cancer
This is a malignant tumour in the prostate which is a gland that sits under the bladder and is involved in production of fluid in the semen.

This is the second most common cancer in men in Australia. One in six Australian men will be diagnosed with prostate cancer by the age of 85. Nevertheless a large percentage of these cancers will be indolent (or slow growing).
The role of the urologist is to diagnose and treat those cancers that are likely to result in premature death (or morbidity).
Screening for
Prostate Cancer
Older age and family history increase the likelihood of having prostate cancer.
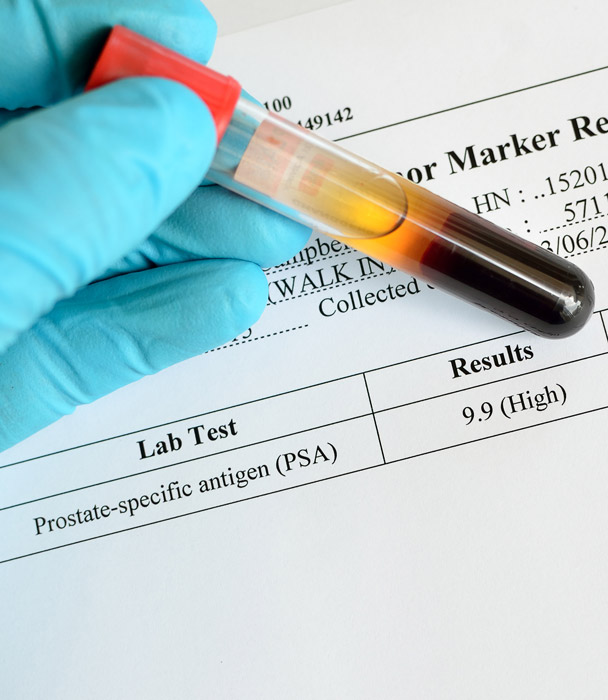
With the advent of a blood test, the PSA (prostate specific antigen), we are now able to diagnose prostate cancers at a much earlier stage than previously and significantly improve survival from prostate cancer.
While it is usually elevated in prostate cancer, it can be elevated in other conditions including benign enlargement of the prostate, infection or inflammation and sexual activity for example.
There has been some controversy about the role of PSA screening in regards to survival and concern about over diagnosis particularly in more slower growing cancers. There have now been a number of large studies that support its role in reducing death from prostate cancer.
There have recently been some developments which have improved the diagnosis of prostate cancers which need treatment (and conversely reduced diagnosis of those that don't).
MRI (Magnetic Resonance Imaging)
The widespread use of this scan has significantly improved the chance of diagnosing more aggressive cancers and importantly reduced the number of unnecessary biopsy procedures. This scan is now medicare rebateable but generally needs two PSA tests one to 3 months apart (or an abnormal feeling prostate on a digital rectal examination). This scan involves around 30 minutes and uses magnetic waves not radiation.
Transperineal prostate biopsies
Traditionally, biopsies were performed through the rectum (back passage) with a small risk of sepsis (widespread infection). A newer technique involves biopsies through the skin in the perineum under the scrotum (ball sac). This generally involves a short general anaesthetic and has the advantage of significantly reducing any infection risk as well as improving the accuracy of biopsies targeting the abnormal areas seen on the MRI.
PET PSMA (prostate specific membrane antigen) scan
This scan allows for more confidently ascertaining that the cancer, particularly if more aggressive, is localised to the prostate or has started to spread. This scan is not always required to proceed with treatment and is reasonably costly.
Active Surveillance
Given that prostate cancer is often slow growing, some cases can be may not need to be treated. Today, the vast majority of low risk prostate cancer is managed by active surveillance. This involves a combination of regular testing of PSA levels, imaging and prostatic biopsies if required.
By doing so, we can avoid unnecessary treatments while at the same time, catch the disease early before distant spread should it worsen. Active surveillance may be suitable for you if you have small volume of disease, low grade disease or multiple medical problems.
Surgery
For localised disease, removal of the entire prostate gland aims to cure patients of prostate cancer.
At the same time the nearby lymph glands can be removed to assess for early potential spread.
This is performed as an open procedure in Wangaratta involving an incision about 10cm from the base of the penis to half way up to the belly button. It generally involves around 3 days in hospital.
This operation can also be performed with keyhole with the assistance of a robot in Melbourne. The advantage of this techniques a shorter hospital stay and a quicker time for recovery (about 2/3 the time). We can facilitate a referral to a Urologist in Melbourne if you would prefer this technique.
Both techniques involve a catheter to be placed in the bladder for 10-14 days to allow the join between the bladder and urethra (water-pipe) to heal. The side-effects from both techniques are similar and generally involve a small risk of significant urinary incontinence and a higher chance of problems with erections (although nerve sparing surgery can be performed if appropriate).

Radiation
The chance of cure with radiation is generally similar to surgery (which are excellent if found early). Radiation can be delivered a few different ways but mostly from outside targeted at the prostate over about 7 and a half weeks. The radiation centres locally are based in Albury or Shepparton.
The side-effects from this are problems with erections and damage to adjacent tissues namely the rectum (bowel) or bladder.

